
The Diaphragm: Beyond Breath (Part 2) Healthy Breathing Mechanics
- Jun 23
- 7 min read
By Gavin Buehler
In our last article we began to take a closer look at the diaphragm and reviewed its anatomy to help us visualize the structure as we dig deeper into its functions. In this article we’ll start to unpack those functions beginning with its well-known purpose of providing breath.
Breathing Mechanics
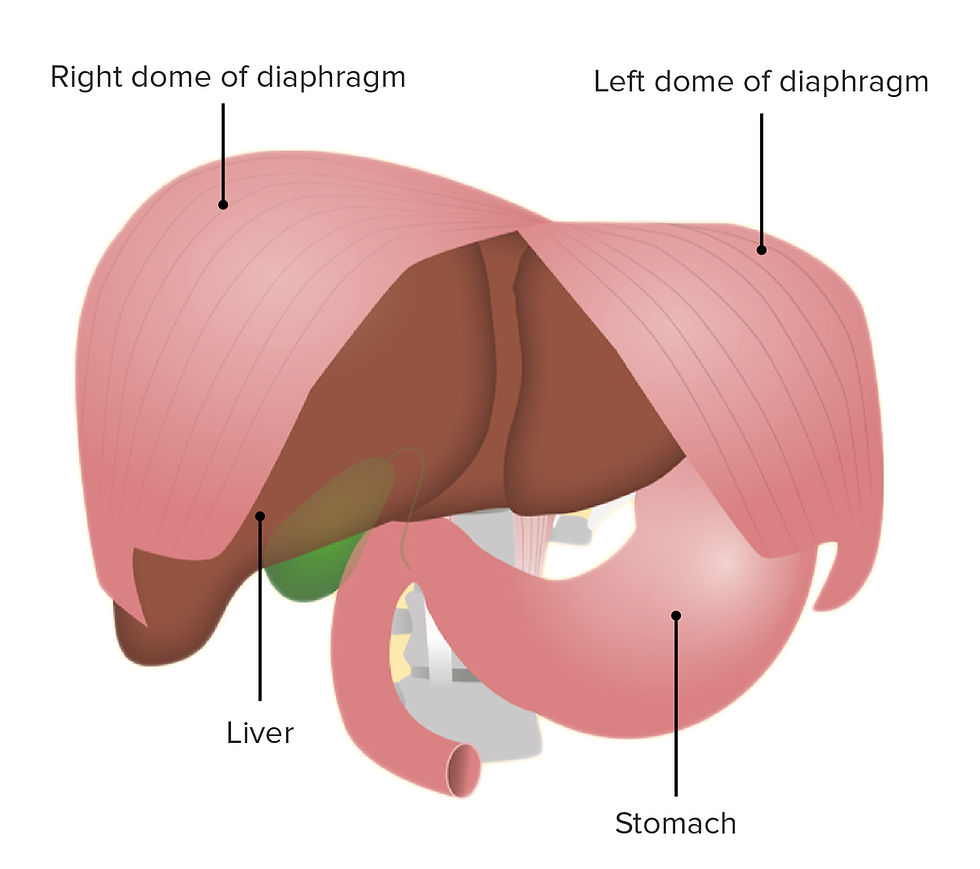
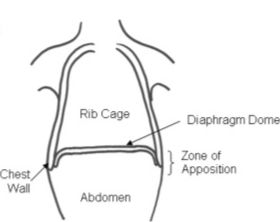
The Diaphragmatic Dome: The dome is the superior (top) curved portion of the diaphragm projecting into the thoracic cavity. The dome is identified as two sections. The right dome (right hemidiaphragm), and the left dome (left hemidiaphragm.) The right section is usually higher because of the liver, and the left dome sits slightly lower because of the heart and stomach.
Inhalation: When the diaphragm contracts the dome descends moving toward the pelvis as it slightly flattens increasing the size and volume of the thoracic cavity. The pressure inside the chest decreases creating a vacuum effect bringing air into the lungs through the trachea. As this occurs, the abdominal contents
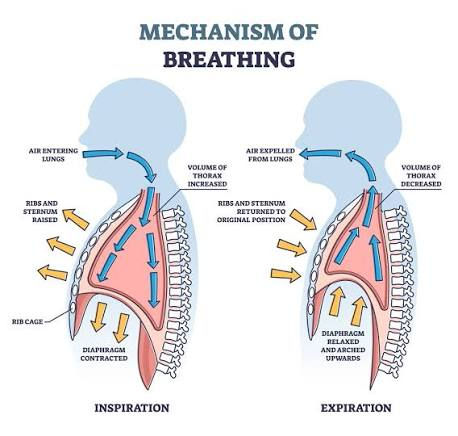
below the diaphragm are displaced downward toward the pelvis and the abdominal wall expands (hopefully in all directions) to also accommodate the displacement of the visceral structures.
Exhalation: When the diaphragm relaxes, elastic recoil and the abdominal pressure that was built from the displacement of the structures below the diaphragm as well as the abdominal wall expansion help the dome return upward.
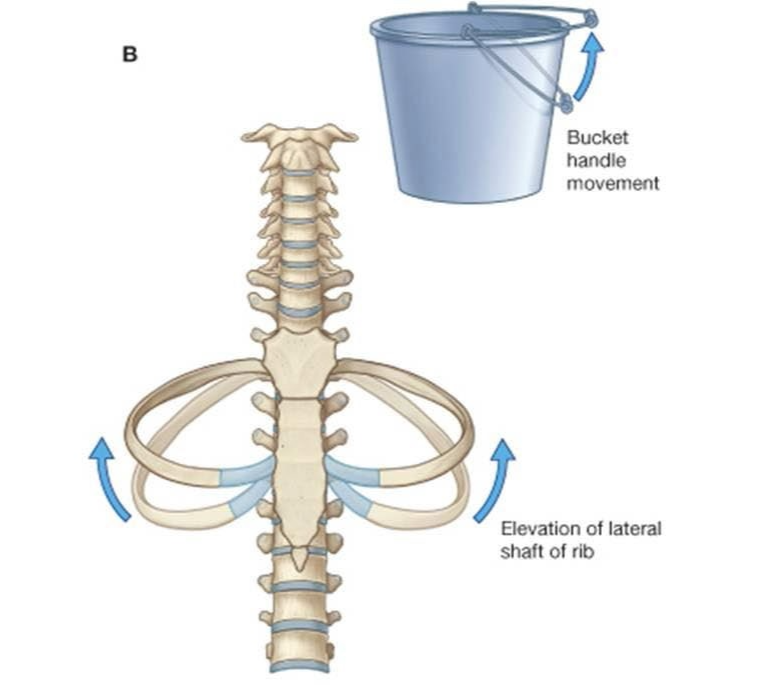
The "Bucket Handle" Effect: This is the commonly used analogy to describe how the lower ribs should move during a breath. As the diaphragm contracts the lower ribs move outward and upward resembling the movement of a bucket handle increasing the width of the thoracic cavity. This movement is also influenced by the costal (rib) muscles. Ideally the main driver of this rib motion should come from healthy diaphragmatic function, however we commonly find excessive contributions from accessory muscles assisting with the expansion of the thoracic cavity. Reliance on the accessory muscles for ribcage expansion with normal breathing can result in overuse of those muscles creating stiffness throughout the thorax. This stiffness limits the ability for expansion and contraction to occur disturbing that “vacuum” effect and can severely limit the flow and volume of air travelling in and out of the lungs. Dependence on these muscles can also lead to the reduction of diaphragmatic activation adding to or creating dysfunction with this structure.
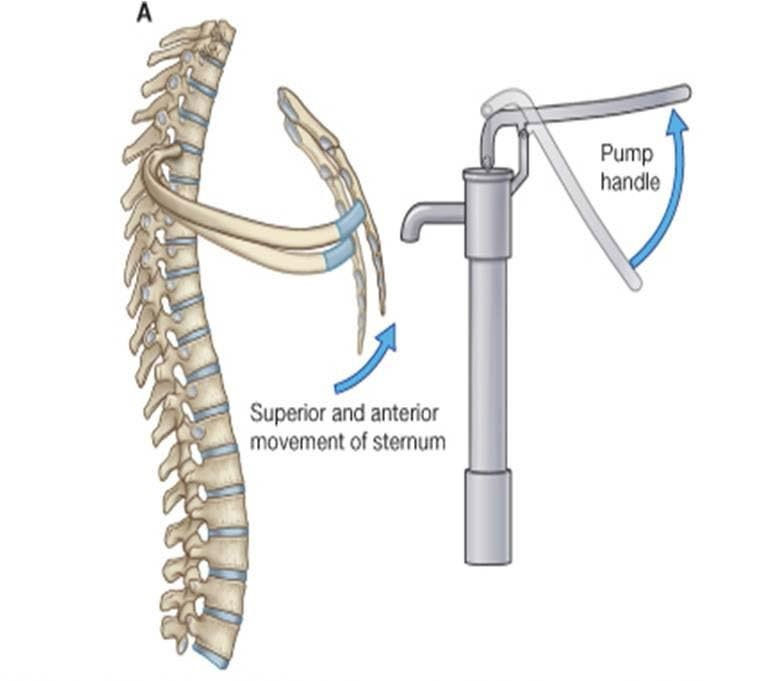
The "Pump Handle" Effect: This is analogy generally used to describe the movement of the upper ribs during a breath. Much like an old water pump handle, the upper ribs move slightly upward and forward during inhalation increasing anterior (front) and posterior (back) chest diameter contributing to greater overall thoracic volume.
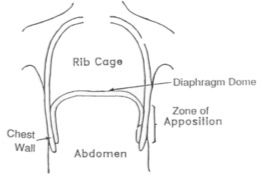
The Zone of Apposition (ZOA)
This is a fancy name for the section of the diaphragm closest to the lower ribs extending vertically toward the central tendon roughly from ribs 7-12. This area is significant because it represents the largest contractile area of the diaphragm. A healthy ZOA allows for maximal diaphragm efficiency as the ability for this area to fully contract pulls the lower ribs outward providing the greatest thoracic volume for air to travel in. This diaphragmatic contraction is also crucial for creating intra-abdominal pressure as the diaphragm descends. This pressure is necessary for healthy diaphragm recoil during exhalation but is also a key component for spinal stability.
ZOA Dysfunction: Since this is the area where the most diaphragmatic movement occurs, it is also the area where we can note if there is a dysfunction with diaphragmatic movement.
A shortness of breath or shallow breathing happens for one of two reasons:
You can’t get air into your lungs for the necessary gas exchanges to take place.
You can’t get the air in your lungs out for fresh air to be able to come in.
The ZOA can lose its movement ability, and the diaphragm can get “stuck” in either the position of inhalation or exhalation. This “sticking” can also occur on just one side of the diaphragmatic dome or both. However, one-sided dysfunction is more common with the left dome due to the position of the liver under the right diaphragm. It is thought that the liver helps maintain healthy ZOA function on the right dome because of its size and position against the diaphragm. Because of this, disruption of the left dome usually happens first and then the right dome will follow in time under prolonged dysfunction.
A healthy ZOA is apparent with good cylindrical expansion and contraction of the ribcage.
What is “good” ribcage movement? In a healthy adult during a deep breath, the ribcage should expand between 1.5” – 2.5”. However, during normal breathing, the consistency of even cylindrical movement is what should be noted throughout the thorax. If there is a section or more that does not move, or the body seems reliant on only one area to expand and contract, there may be an issue with the ZOA.
“Stuck in inhalation” – This position is apparent when the lower ribs remain in that raised bucket handle position and appear flared out. The diaphragm is stuck in its contracted position where it is flatter expanding the ribcage. In this case, more air can’t be taken into the lungs because the ability for the diaphragm to relax, properly recoil and dome to push the old air out is not available. This can lead to excessive use of accessory breathing muscles such as the intercostals (rib muscles), pecs, lats, traps, scalenes and more, trying their hardest to expand and contract the thoracic cavity. This is usually where we see what is called “apical” breathing where only the upper chest appears to move because of those accessory muscles doing most of the work. Of course, with those muscles overworking, they will also become stiff and achy and lose their ability to contract and relax. This is the “stuck” position is quite common. It’s the loss of being able to exhale fully rather than the inhale being the limiting factor.
A notable side effect of this dysfunction is that since the diaphragm is stuck in its flattened position, it is also placing a constant pressure on all of the abdominal viscera (organs, guts) below it as well as the pelvic floor and outward pressure into the abdominal wall. This constant pressure may cause disruption of the normal functioning in those structures. Now we can really start to see just how important proper diaphragmatic function is for a global balance of functions throughout the entire body.
“Stuck in exhalation” – Opposite to the above example, this position is apparent when the lower ribs appear to be pulled down and in or just don’t move out of the down and in position during inhalation. In this case the diaphragm is “stuck” in its lengthened position domed and the ZOA has lost its ability to contract and shorten to expand the thoracic cavity and allow air into the lungs. The results of this position are similar to the above example where the accessory muscles kick into overdrive and the presentation of “apical” breathing occurs.
With the constant loss of intra-abdominal pressure, normal operations of the visceral structures may be affected just like if there is too much constant pressure, and spinal stability is very compromised in this position with the lack of intra-abdominal pressure.
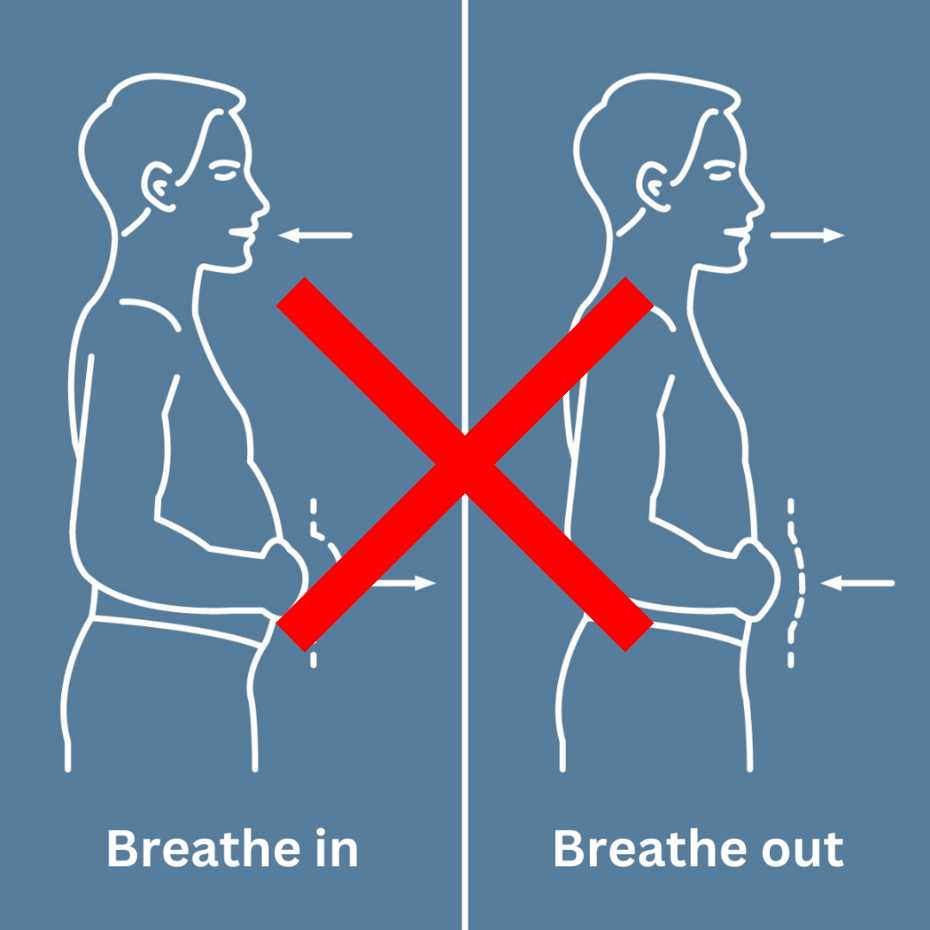
Belly Breath – Let’s address the infamous “belly breath” cue. While well intended, this is a cue that should be taken into consideration on a case-by-case basis. Based on the anatomy, we can see that our lungs are housed in the thoracic cavity within the ribcage above the belly. Belly expansion happens because the diaphragm descends with the goal of drawing air into the lungs. This descension of the diaphragm squishes the viscera (belly contents) creating expansion of the belly. Belly expansion is a side effect of breath NOT the desired effect. Belly breathing is not diaphragmatic breathing.
Belly only breathing is another sign that the ZOA may be compromised. Whether stuck with the ribs expanded or down and in, the ability to expand and contract the ribcage is gone but there will still be some movement of the diaphragm up and down. Only having one axis of movement limits thoracic volume and defers more pressure toward the abdominal wall, viscera and pelvic floor.
Proper diaphragmatic breathing is expressed when there is a full cylindrical expansion of the entire thorax. We want to see the ribcage expand evenly because that is where our lungs are not our belly, but we will also see expansion through the belly as the diaphragm descends compressing the viscera. The goal should never be to force the belly out.


The Lymphatic System and the Diaphragm
A healthy breathing rhythm is crucial for many reasons, but this is a good spot to highlight its importance for the lymphatic system. The lymphatic system is a vital network of vessels, nodes, and organs that act as the body’s drainage and defense system. It circulates a fluid called lymph, removes toxins and waste, absorbs fats, and houses immune cells to protect against infections and diseases. It is critical for overall health and survival. This system does not have its own built in pump mechanism to circulate its fluid. Two of its most important pumping mechanisms come from breath and skeletal muscular contractions. A disruption of a healthy breathing pattern can dramatically impact proper lymph fluid circulation lowering immune function and leaving the body exposed. This is also why regular exercise or movement is so valuable for immune support as it is one of the primary pumps for lymphatic circulation.
We can really start to see the dramatic effects that the diaphragm can have on the entire body beyond its “main” function of breath. It a foundational pillar for overall health.
Stay tuned for part 3 as we dig even deeper into diaphragmatic connections and start to look at its structural impact and reach through fascia.
Did you like this article and find it helpful? Please consider sharing it. Thank you!
As always, these articles and videos are for entertainment and educational purposes only. Please consult a health professional before attempting new exercises or protocols, as the following suggestions may or may not be appropriate for you.


Comments